1. Prepared by Curtis Gravenmier MD and reviewed by Heba Mostafa MBBCh, PhD, D(ABMM)
An adult patient with metastatic carcinoma was brought to the hospital after new onset neurologic symptoms and weakness. Their medications included lisinopril, metoprolol, apixiban, semaglutide, and levothyroxine, as well as the PD-L1 inhibitor atezolizumab. Physical examination, routine chemistry, blood counts, and a urine drug screen were unremarkable, and the patient was admitted to oncology for further evaluation.
During the next 24 hours, additional neurologic symptoms became apparent. Magnetic resonance imaging of the brain offered no explanation, but importantly showed no mass or abnormal enhancement. An electroencephalogram was without seizure activity.
Lumbar puncture demonstrated a lymphocytic pleocytosis and elevated total protein (81.2 mg/dL), prompting a battery of tests in the microbiology laboratory. These uncovered no evidence of enterovirus, herpes simplex viruses 1 and 2, varicella zoster virus, cytomegalovirus, West Nile virus, Cryptococcus antigen, or Treponema pallidum. However, human herpesvirus 6 (HHV-6) was detected in the patient's cerebrospinal fluid at a level of 630 copies/mL using real-time quantitative polymerase chain reaction (RTq-PCR). This sole positive finding was reproduced using the patient's plasma, which showed 242,000 copies/mL.
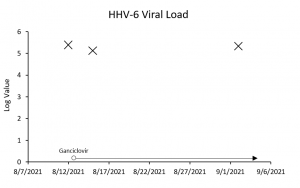
The symptoms resolved without specific intervention. Nonetheless, the patient was discharged with a 3-week regimen of ganciclovir for presumed HHV-6 meningoencephalitis. A graph of HHV-6 plasma PCR, performed twice after the initial test, is shown below. The patient remained asymptomatic despite persistently elevated levels of viral DNA.
 Question:
Question:Which of the following best explains the persistently elevated HHV-6 plasma PCR in this patient?

