1. Presented by Caitlin Alexander, MD, MPH and reviewed by Sean Zhang, MD, PhD.
An adult patient with a history of receiving chemotherapy developed a fever of 38.3°C in the setting of neutropenia. The patient denied cough, shortness of breath, GI symptoms, or dysuria. Physical exam was notable for clear lungs to auscultation. Of note, the patient has an extensive domestic and international travel history. Complete blood count showed WBC 0.42 K/mm3 (ANC 0.02 K/mm3). Chest CT revealed bilateral multifocal patchy and consolidative ground glass opacities consistent with multifocal pneumonia.
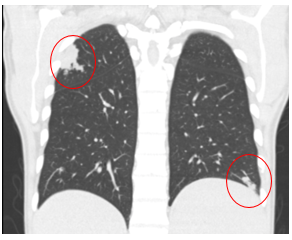
Figure: CT imaging showed multiple pulmonary nodules.
The patient had been on valacyclovir and posaconazole for prophylaxis during chemotherapy, and was started on empiric therapy with vancomycin and piperacillin-tazobactam.
Laboratory Results:
Blood and urine cultures showed no growth. Respiratory viral NAT testing was negative. Galactomannan and Beta-D-Glucan tests were negative. Antigen testing for Legionella, Streptococcus pneumoniae, Histoplasma, and Cryptococcus, as well as Blastomyces antibody testing were performed, and were all negative except Cryptococcal antigen, which was positive in serum by lateral flow assay.
A bronchoalveolar lavage (BAL) was performed, and specimens were sent for bacterial and fungal culture. The bacterial culture grew a yeast-like colony. The yeast was tested by matrix-assisted laser desorption-ionization time-of-flight mass spectrometry (MALDI-TOF), and identified as Cryptococcus gattii, which was then DNA sequenced and confirmed.
A lumbar puncture was performed. Opening pressure was not elevated, WBC was 1 per mm3, glucose was 76 mg/dL, and protein was 22.3 mg/dL. Bacterial and fungal CSF cultures were negative, no organisms were seen on calcofluor white stain, and cryptococcal antigen testing by lateral flow assay was negative.
Question:
Cryptococcus gattii is common in which areas of North America?

